Preserving the Direct Contracting Model for Medicare Beneficiaries

Medicare Direct Contracting is a voluntary accountable care organization (ACO) model that builds on lessons learned from the Medicare Shared Savings Program (MSSP) and the Next Generation ACO models. Healthcare providers support Direct Contracting because it shifts payment away from underlying fee-for-service (FFS) incentives that encourage volume of services over the quality and value of care. Participating Direct Contracting providers receive capitated or value-based payments, while other ACO models continue to rely on FFS payments with payment reconciliation.
While Direct Contracting supports the bipartisan drive to value-based care, some have called for ending the model. Premier has joined roughly 220 other organizations in calling on CMS to continue with this program that aims to deliver results for beneficiaries and the government. With improvements, the Direct Contracting Model can further galvanize ACOs that are improving care for their patients and lowering healthcare spending.
Canceling Direct Contracting will be a wasted investment for providers and the government.
- Providers already operating in this model make significant up-front investments to enter the model and innovate care delivery.
- Participants who joined in the second year of the model previously participated in the Next Generation ACO model. This reflects more than six years of commitment to value-based arrangements.
Misconceptions have led to a call for the end of the Direct Contracting model. Here are the facts.
- Direct contracting entities (DCEs) are unable to ratchet down care to achieve maximal savings. As with other ACO models, DCEs are unable to use prior authorization to slow or prohibit beneficiaries from seeking care. Beneficiaries can still see any Medicare provider and seek all needed care.
- DCEs are unable to automatically enroll patients. As with other ACO models, beneficiaries can voluntarily participate with the DCE or are aligned if they receive most of their primary care from a participating provider in the DCE.
- DCEs cannot switch patients from Medicare to Medicare Advantage. Direct Contracting is a traditional Medicare model that is built on top of fee-for-service that gives provider participants the option to receive capitated payments or other downstream payment arrangements. Providers have valued the opportunity to receive capitated payment as with other models like Primary Care First.
- The model does not incent gaming of risk scores. Patient risk scores are critical to assure adequate payment based on the health of the patient and patient population. Every value-based care model should use a consistent coding and documentation methodology and be monitored for compliance.
Like other ACOs, Direct Contracting gives beneficiaries access to enhanced benefits.
- Participating providers are able to coordinate care across the continuum, ensuring that beneficiaries receive the right care at the right time in the right place.
- Participating providers have enhanced access to data that allows for interventions targeted to the individual and community.
- Participating providers can provide more equitable care with enhanced coordination and access to community supports.
Rather than end the model, CMS should make changes to improve the model to encourage provider participation.
- Align requirements for Direct Contracting participant organizations with MSSP.
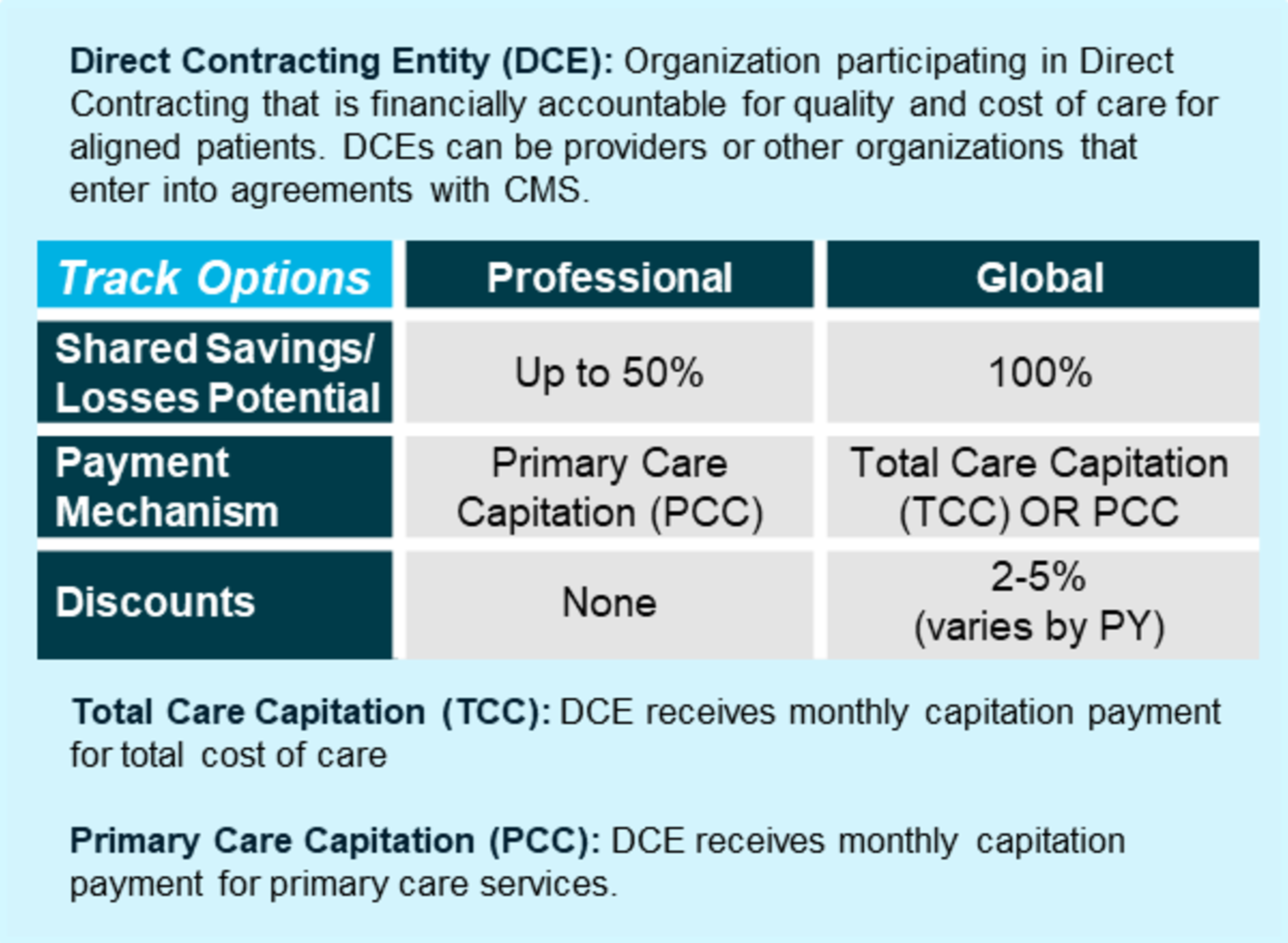
- Set more reasonable discounts to ensure providers receive adequate payment under the Global Track.
- Increase opportunities for shared savings under the Professional track to be comparable to higher risk tracks in MSSP.
- Apply consistent methodologies and polices across participants to ensure providers have the same opportunity to participate as non-providers.
The insights you need to stay ahead in healthcare: Subscribe to Premier’s Power Rankings newsletter and get our experts’ original content delivered to your inbox once a month.